Brain tumor
Brain tumor also often referred to as brain cancer is when a collection of cells within the brain become cancerous and begin to grow in an abnormal fashion and form a tumor. There are two wide classifications of tumors: malignant tumors and benign non-tumorous tumors.
These may be classified further into primary tumors, which start in the brain, and secondary tumors that most commonly have arisen from tumors located outside the brain known as brain metastasis tumors. All types of brain tumors can present symptoms that vary according to the tumor size and area of the brain involved. Where they do present, symptoms may include headaches seizures vision disturbances vomiting and mental change. Inability to walk speak with sensations or to be unconscious may be other symptoms.
The cause of most brain tumors is unknown although up to 4% of brain cancers may be at least partially caused by radiation from CT scans. Unconventional risk factors include exposure to vinyl chloride Epstein Barr virus ionizing radiation and genetic syndromes such as neurofibromatosis tuberous sclerosis and von Hippel Lindau Disease. Studies of mobile phone exposure have not been shown to prove a clear risk.
The most common types of primary tumors in adults include meningiomas and astrocytomas such as glioblastomas. In children the most common is a malignant medulloblastoma. Diagnosis is usually by medical examination and computed tomography or magnetic resonance imaging. The diagnosis is then typically established with a biopsy. The tumors are graded based on the findings into different grades of severity.
Treatment may be a combination of surgery, radiation and chemotherapy. If a seizure is present anticonvulsant drugs may be required. Dexamethasone and furosemide are medications that can be administered to minimize swelling in the tumors vicinity. A few tumours are very slow-growing and only require observation and possibly no other treatment.
Immunotherapy or the utilization of one’s own immune system is being researched. Cancerous tumour prognoses vary considerably depending on the tumour type and stage of spread at diagnosis. Although benign tumours develop in one region they may also be harmful to life based on their size and location. Malignant glioblastomas usually have extremely poor prognosis while benign meningiomas usually have good prognosis. The five year median survival rate for all the malignant brain cancers in the United States is 33%.

Causes of brain tumor
A known cause of brain cancers is ionizing radiation. Approximately 4% of the brain cancers in the general population result from CT scan radiation. For brain cancers occurring after CT scans with delays of 2 years or more it has been approximated that 40% result from CT-scan radiation. The risk for brain cancer is dose dependent with relative risk increasing by 0.8 for each 100 gray of ionizing radiation exposure. It would require approximately 6391 people at this dose to cause 1 case of brain cancer. Ionizing radiation to the head as a treatment for other cancers is another risk factor for the development of brain cancer.
Deletions and mutations of tumor suppressor genes such as P53 are thought to be the etiology of some types of brain tumor. Genetic diseases such as Von Hippel Lindau disease tuberous sclerosis multiple endocrine neoplasia and neurofibromatosis type 2 carry a high risk of brain tumors. Celiac disease sufferers are at slightly higher risk of brain tumors. Smoking may increase the risk but data on this are unclear.
Although research has not yet indicated any connection between mobile phone or cell phone radiation and the development of brain tumors the World Health Organization placed mobile phone radiation on the IARC scale under Group 2B possibly carcinogenic. The hypothesis that using cell phones is capable of resulting in brain cancer can be based on epidemiologic studies that mentioned elevated glioma risk among high users of wireless phones.
When they conducted their research cell phones existed. Third generation telephones that exist now emit about 1% of the energy amount that the old GSM telephones emitted and thus the conclusion drawn that there existed a correlation between the use of cell phones and a higher risk of brain cancer is not something that resulted from the usage of cell phones at present.
Diagnosis of brain tumor
No characteristic symptom or sign of brain cancer but the presence of a group of symptoms and exclusion of other etiologies is suggestive of a brain tumor. History is of assistance in the diagnosis. Examinations with clinical and laboratory will be utilized to exclude infection as a cause of the symptoms.
Brain tumors as opposed to tumors in the rest of the body pose difficulty in diagnosis. Normally radioactive tracers are taken up in significant quantities in tumors due to the high activity of tumor cells to allow radioactive scintigraphy of the tumor. The majority of the brain is otherwise isolated from blood by the blood brain barrier a membrane with tight regulation of what can be brought into the brain.
A tremendous number of tracers which would otherwise find their way into tumors in other parts of the body with comparative ease would be barred from entering brain tumors until tumor-induced BBB disruption. Disruption of BBB can be seen readily by MRI or CT scan and therefore represents the main diagnostic finding for malignant gliomas meningiomas and metastases to the brain.
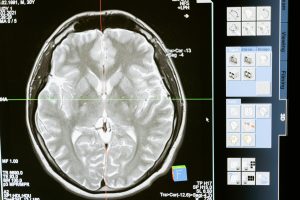
Imaging of brain tumor
The diagnosis of brain tumors leads the field with the use of medical imaging. Invasive and often dangerous initial imaging methods such as pneumoencephalography and cerebral angiography have been substituted by noninvasive high resolution imaging methods especially magnetic resonance imaging and computed tomography scans. Contrast-enhanced MRI is the imaging procedure of choice in the diagnosis of brain tumors. Glioblastomas are usually enhanced with contrast on T1 MRI weighted MRI imaging and on T2 with FLAIR imaging as hyperintense cerebral edema. Low grade gliomas are generally hypointense on T1 MRI and hyperintense with T2 with FLAIR MRI. Meningiomas are generally homogenously enhanced with dural thickening on MRI.
Different Types of MRI Scans
Magnetic Resonance Angiography scans the blood vessels in the brain. In the diagnosis of brain tumors MRAs are usually done pre-operatively to help surgeons have a better sense of the vasculature of the tumor. For example in research, surgeons were able to distinguish benign brain tumors from malignant brain tumors based on the vessel shapes of the blood vessels that were recovered from MRA. Though not required, some MRA will inject contrast agent gadolinium into the patient to gain a better view
Magnetic Resonance Spectroscopy measures the metabolic changes or chemical changes in the tumor. The most common MRS is proton spectroscopy whose frequency is measured in parts per million. Gliomas or brain tumors are also characterized by varying spectra from normal brain tissue in that they have elevated choline content and decreased N acetyl aspartate signals.
Use of MRS in the diagnosis of brain tumors can help doctors decide on the nature of the tumor and its malignancy. For example, benign brain tumors or meningioma have high concentrations of alanine. It can also be employed to distinguish brain tumors from scar tissues or necrotic tissues due to previous radiation therapy that does not have the high choline content of brain tumors and from tumor-simulating lesions such as abscesses or infarcts.
Treatment of brain tumor
Treatment options are commonly assessed by the medical team, and they inform the individual affected and the family accordingly. There are various treatments depending on tumor location and type, and treatments can be coupled to achieve the best survival prospect
Surgery complete or subtotal resection of the tumor for the purpose of removing as many of the tumor cells as possible.
Radiotherapy the most common therapy of brain tumors the cancer is treated by exposing the tumor to beta x rays or gamma rays.
Chemotherapy a therapy for cancer but it is not always used in treating brain tumors since the blood brain barrier may prevent some medicines from reaching the cancer cells.
Experimental treatments are available in the form of clinical trials.
Survival with primary brain tumors is influenced by tumor type age functional status of the patient surgical resection and other variables specific to the individual case.

Surgery
Surgical extirpation of as much tumor as possible containing contrast enhancing tissue gross total resection is associated with better overall and progression free survival in glioblastoma patients. Gross total resection is normally required in other intracranial tumors also. Minimal access procedures are the common trend nowadays in neurosurgical oncology. The main aim of surgery is the removal of as much of the tumor cells as possible with maximum removal being the best outcome and cytoreduction of the tumor can otherwise be done. Due to the infiltrative nature of glioblastomas total resection is usually not feasible and recurrence after surgery usually occurs with recurrence usually occurring at about 7 months after surgery.
The majority of meningiomas except some at the skull base are successfully removed by surgery. The majority of pituitary adenomas are resectable through surgery typically a minimally invasive procedure through the nasal route and skull base trans nasal trans sphenoidal approach. Large pituitary adenomas require a craniotomy skull opening for removal. Radiotherapy including stereotactic approaches, is reserved for those not amenable to surgery.
Some metastatic tumors are managed with radiotherapy and chemotherapy but not surgery, and the prognosis in such cases depends on the primary tumor and is generally poor.
Radiation therapy
The goal of radiation therapy is the killing of tumor cells without harming normal brain tissue. In traditional external beam radiation therapy several courses of traditional dose fractions of radiation are given to the brain. The process is done again for 10 to 30 treatments based on the type of the tumor. This additional treatment adds some patients to get improved outcomes and longer survival rates.
Radiosurgery is a type of therapy in which computerized calculations are employed to focus the radiation at the tumor location without increasing the dose of radiation on the surrounding brain tissue. Radiosurgery may be employed in conjunction with other treatments as an adjuvant or as the primary method of treatment for certain tumors.
Radiotherapy is the most common treatment of secondary brain tumors. The radiotherapy dose depends on the size of the brain region affected by cancer. Standard external beam whole brain radiotherapy treatment whole-brain irradiation may be indicated if there is a possibility of other secondary tumors developing in the future. Stereotactic radiotherapy is usually indicated in cases with fewer than three small secondary brain tumors. Radiotherapy may be given after or in some instances as a substitute for tumour resection. Methods of radiotherapy used for brain cancer include external beam radiation therapy, the most common, and brachytherapy and proton therapy the latter specifically used for children.